Marlboro.
Whether you smoke or not, what do you think of when you hear that word? Cowboys and the American West, right? I grew up in 1970s suburbia and have been on a horse once in my life. I have more to with the American West than Marlboro!
Where does Marlboro come from? Marlboro is owned by a British corporation, Philip Morris. The name comes from a street in London called Great Marlborough on which its factory was first situated. It originally started as a cigarette for women in the 1920s, and was known with the tagline, Mild as May, because their first “smokeperson” was not the Marlboro Man, but rather the famous movie star Mae West.
As can be seen in the ad, smoking was considered a feminine activity and not considered “manly.” In the 1950s, Philip Morris wanted to change their marketing to men and worked with Leo Burnett of New York to create the Marlboro Man to market to men. The cowboy was chosen and the rest is history. Instead of thinking of a street in London, England, we associate Marlboro with the American cowboys. That is the power of advertising and brand identification.
Marketing does not take place on a billboard, on a television station, or in a magazine. It takes place in one’s individual consciousness. It creates a mental image that the viewer identifies with or wants to identify with.
As Al Reis and Jack Trout state in
Marketing_Warfare (p . 44) “Marketing battles are fought in a mean and ugly place. A place that’s dark and damp with much unexplored territory and deep pitfalls to trap the unwary. The mind is the battleground. A terrain that is tricky and difficult to understand. The entire battlefield is just 6 inches wide. This is where the marketing war takes place. You try to outmaneuver and outfight your competitors on a mental mountain about the size of a cantaloupe. A marketing war is a totally intellectual war with a battleground that no one has ever seen. It can only be imagined in the mind, which makes marketing warfare one of the most difficult disciplines to learn.”
It is the power of advertising to effect behavioral change in an individual and a society that most interests me. Personally, I believe advertising has led to some remarkable changes in American life in terms of one’s health. From my perspective we can see this in how it has changed our social norms.
For instance, I believe the greatest cause of increase in our calories as a country is related to increase in portion sizes. Supersized meals and supersized sodas now look normal. A “typical” (based on RDA values) individual serving size now appears small. This is not because the serving size has changed, but because how we perceive them has changed. A great deal of this was accomplished through very successful marketing by different organizations. For instance, as detailed in Greg Crister's
Fatland. David Wallerstein, who was a director at McDonald's corporation, was first to suggest to the founder, Ray Kroc, to introduce supersized fries. He argued that it was a
values proposition. People felt (and bought) that they were getting an increased
value for the extra money they spent on the larger fries. The consumer thus doesn't feel they are suffering from gluttony but rather they convince themselves they are being "frugal" shoppers by paying a little more for a much larger portion. Meanwhile the franchisee is able to spend just a few extra pennies to create the supersized meal, with the extra charge being primarily pure profit.
This has had a caloric effect on the individual consumer. From
Fatland, p. 28: "By the end of the century, supersizing --the ultimate expression of the value meal revolution -- reigned. As of 1996, some 25 percent of the $97 billion spent on fast food came from items promoted on the basis of either larger size or extra portions. A serving of McDonald's French fries had ballooned from 200 calories (1960) to 320 calories (late 1970s) to 450 calories (mid 1990s) to 540 calories (late 1990s) to the present 610 calories (2003). In fact, everything on the menu had exploded in size. What was once a 590-calorie McDonald's meal was now...1550 calories. By 1999 heavy users -- people who eat fast food more than twenty times a month -- accounted for $66 billion of the $110 billion spent on fast food...Kids had come to see bigger everything -- bigger sodas, bigger snacks, bigger candy, and even bigger doughnuts -- as the norm; there was no such thing as a fixed immutable size for anything, because anything could be a made a lot bigger for just a tad more."
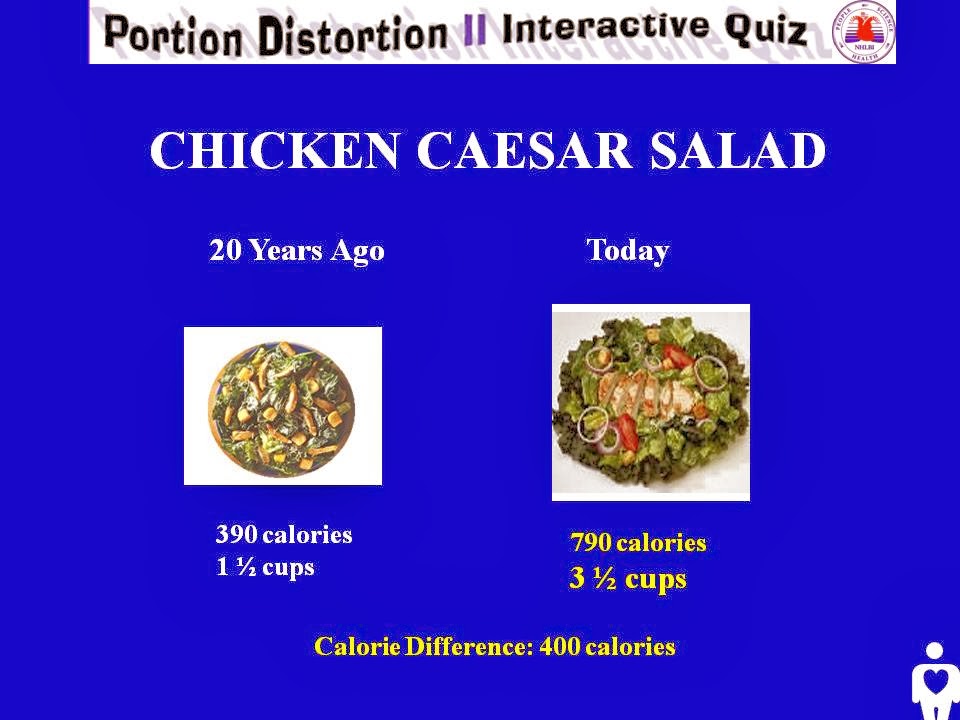
We can see this change from the National Institute of Health Portion Distortion
website, regarding how portion sizes have changed over 20 years from 1984 to 2004
Just look at the first picture of the coffee. I believe it is almost impossible to view the coffee on the left as "small." However, if we went back 20 years, we may have looked at the coffee on the right as "huge." The latter view is probably a more correct one from a caloric perspective. Here are some more examples of portion distortion
But how do we go back? Our appetite in a variety of ways has fundamentally changed, and we've entered a "new normal." This blog is not a criticism of brand marketing. Rather it is to help us become aware of its impact. We often state how hard it is to effect behavioral change, yet many companies are quite effective at creating it and we may have something to learn from them.
Perhaps we can use similar marketing techniques to create a healthier society, but the question is, how? This post may lead to more questions in this regard than answers; however, I think it may be beneficial to study how marketers can move products and in so doing effect behavioral change. It often requires an understanding not of rational concerns, but emotional ones. We must be able to connect with the individual -- understand and appreciate his/her anxieties, fears and desires. Perhaps, if we are honest with ourselves, we can learn a great deal from this marketing warfare to truly effect a healthier society.










{kind=link}
{kind=link}